Red Light Therapy Glossary: Every Term Explained in Plain English
Key Insights
- The two numbers that actually matter: wavelength and irradiance. Wavelength (measured in nanometers, nm) determines how deep the light penetrates and what it affects — skin surface vs muscle vs joint. Irradiance (measured in mW/cm²) determines how strong the dose is at a given distance. A device can have the “right” wavelength on paper and still underdeliver if irradiance is too low — these two numbers work together, not separately.
- “Photobiomodulation” is the term researchers use; “red light therapy” is the consumer term for the same thing: If you’re reading clinical studies (which this site links to throughout), you’ll see “photobiomodulation” or “PBM” — it’s the same mechanism, same wavelength ranges, just the formal name used in peer-reviewed literature versus marketing.
- Dose (J/cm²) is wavelength × irradiance × time — and it’s the number that actually predicts results: Two devices with identical wavelengths can deliver very different doses depending on irradiance and how long you sit in front of them. This is the concept that connects “what device should I buy” to “how long should my sessions be” — they’re not separate questions.
- FDA “cleared” doesn’t mean “clinically proven for your specific goal.”: FDA Class II clearance is a real regulatory designation, but it’s a safety and equivalence classification, not a guarantee of efficacy for every claim a brand makes. Understanding what clearance actually certifies helps you read product pages more accurately.
- The honest context: Manufacturers sometimes use technical-sounding terms loosely — “clinical grade,” “medical grade,” and similar phrases aren’t standardized terms with enforced definitions in this industry. This glossary focuses on terms that do have precise technical meanings, specifically so you can tell the difference between a spec that means something and a phrase that’s just marketing language.

Understanding Red Light Therapy in Practice
Red light therapy is often discussed in theory, but its real-world application depends on measurable parameters like wavelength and exposure. I tested multiple RLT setups using a professional spectrometer to better understand how the therapy works in practice.
Core Concepts (Start Here If You’re New to RLT)
Photobiomodulation (PBM)
The formal, scientific name for what red light therapy devices do. Photobiomodulation refers to the use of red and near-infrared light to influence cellular activity — primarily through effects on mitochondria, the energy-producing structures inside cells. When you see “photobiomodulation” in a study and “red light therapy” on a product page, they’re describing the same underlying mechanism. PBM is the term you’ll see throughout the research summarized in our main RLT guide.
Wavelength (nm)
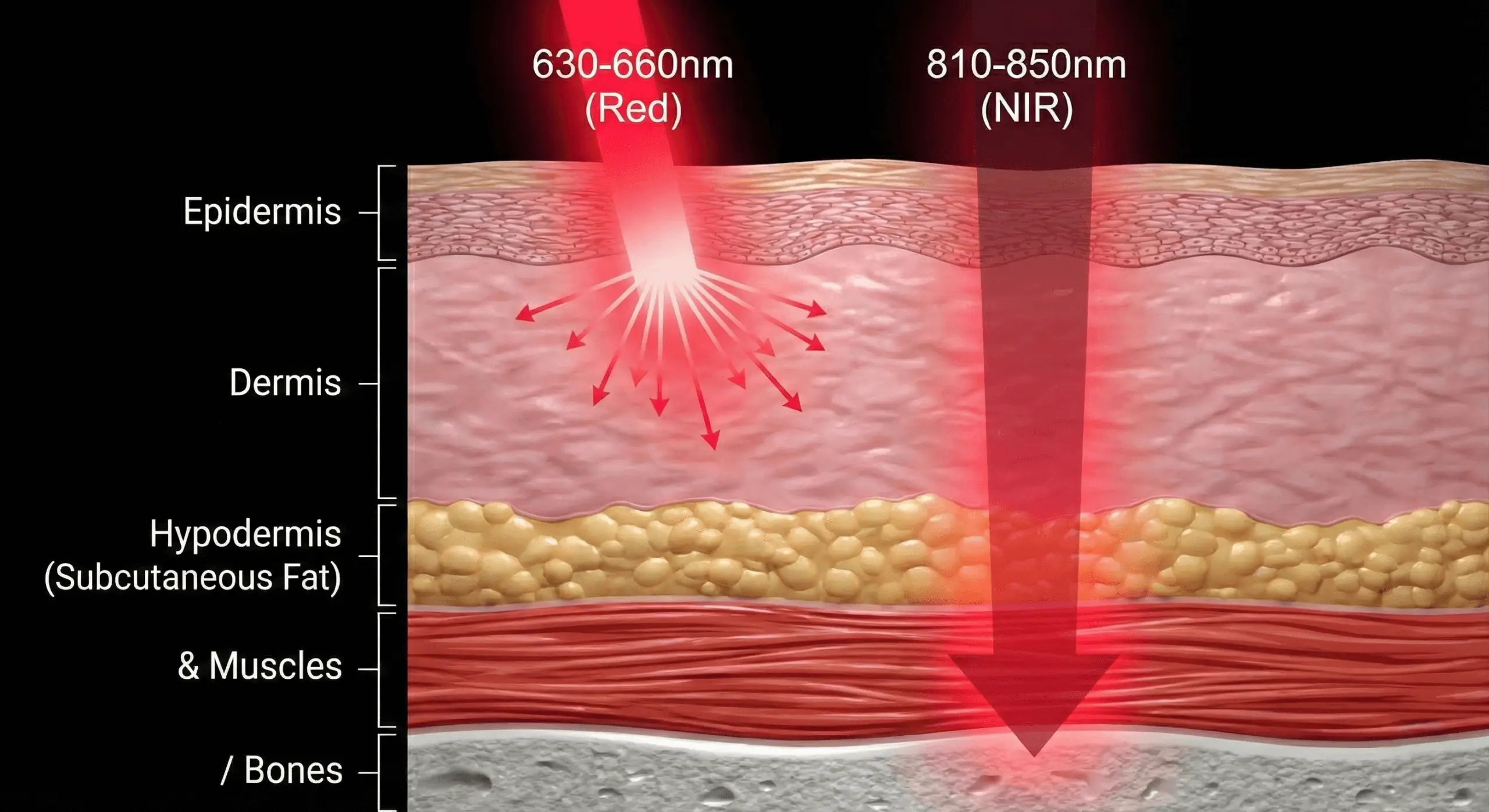
Measured in nanometers, wavelength determines two things: how deep the light penetrates into tissue, and which biological processes it primarily affects. Shorter wavelengths (like 415nm blue light) interact mainly with skin surface — this is the range used for acne treatment. Longer wavelengths in the red and near-infrared range (630–850nm) penetrate progressively deeper, reaching muscle, joints, and connective tissue. The 660nm vs 850nm breakdown covers the two most clinically-supported wavelengths in detail — these are the numbers to check first on any device spec sheet.
Near-Infrared (NIR)
The portion of the light spectrum just beyond visible red light — roughly 800–1100nm — invisible to the human eye but still penetrating tissue. NIR wavelengths (most commonly 850nm) go deeper than visible red light, which is why panels marketed for muscle recovery, joint pain, or deep tissue work emphasize NIR alongside red.
Irradiance (mW/cm²)
This is the intensity of light hitting a surface, measured in milliwatts per square centimeter. Irradiance is distance-dependent — it drops significantly as you move further from a panel, which is why most protocols specify a distance (commonly 6–12 inches) alongside a session length. A device with a high irradiance rating at 6 inches might deliver a meaningfully lower dose at 18 inches, even though the panel itself hasn’t changed. When a product page doesn’t publish irradiance data, it’s difficult to verify whether a session at the recommended distance and duration actually delivers a clinically relevant dose — this is one of the most common gaps between marketing copy and verifiable spec.
Fluence / Dose (J/cm²)
Fluence — often just called “dose” — is the total energy delivered to tissue over a session, measured in joules per square centimeter (J/cm²). It’s calculated from irradiance × time. This is the number that research protocols actually specify (e.g., “4–6 J/cm² for skin applications”), because it captures both how strong the light is and how long you were exposed to it. Two very different combinations — high irradiance for a short time, or lower irradiance for longer — can deliver the same dose. The dosing guide translates this concept into practical session lengths by goal.
Chromophore
A chromophore is a molecule that absorbs specific wavelengths of light — in photobiomodulation, the primary chromophore of interest is cytochrome c oxidase, an enzyme complex found in mitochondria. When red and near-infrared light is absorbed by this chromophore, it influences cellular energy production (ATP synthesis), which is the proposed foundational mechanism behind most of PBM’s downstream effects — reduced inflammation, improved circulation, and tissue repair signaling.
Device & Spec Terms (What to Check Before Buying)
Continuous vs Pulsed Light
Most consumer red light therapy panels emit continuous (constant) light output during a session. Pulsed light — where the LED rapidly switches on and off at specific frequencies — is used in some research protocols and a smaller subset of devices, with some studies exploring whether specific pulse frequencies offer advantages for certain applications. For most at-home use cases, continuous output from a device with verified wavelength and irradiance is the well-established standard; pulsed-light claims are worth scrutinizing for actual supporting evidence rather than assuming “more advanced” automatically means “more effective.”
FDA Clearance (Class II)
FDA Class II clearance (also called 510(k) clearance) means a device manufacturer has demonstrated their product is “substantially equivalent” to an already-legally-marketed device in the same category. It’s a real regulatory designation that indicates a baseline of safety review — but it’s important to understand what it does not mean: clearance doesn’t independently verify every specific claim a company makes about results, and it doesn’t mean the FDA has tested the device’s effectiveness for every condition mentioned in marketing materials. When you see “FDA-cleared” on a red light therapy device, it’s a meaningful safety signal, not a substitute for checking the underlying research for your specific goal.
Coverage Area
The physical surface area a device can treat in one session without repositioning. This sounds simple but is one of the most misrepresented specs in the category — a panel’s name (e.g., “full-body panel”) doesn’t always match its actual coverage geometry at a realistic treatment distance. The full-body panel guide goes into how to evaluate this claim against a panel’s actual dimensions.
Treatment Distance
The recommended distance between the device and skin, typically specified in inches. This number isn’t arbitrary — it’s directly tied to the irradiance rating, since intensity drops with distance. A device’s published irradiance is usually only accurate at the specified treatment distance; standing further away than recommended delivers a meaningfully lower dose than the spec sheet implies, even with an otherwise identical session length.
Session Frequency
How often a protocol recommends using a device — daily, several times per week, etc. — as distinct from session duration (how long each session lasts). Frequency and duration are both part of total weekly dose, and most goals have published frequency guidelines worth following rather than guessing. The common mistakes guide covers how inconsistent frequency is one of the most common reasons people don’t see expected results.
Wavelength-Specific Terms by Use Case
415nm (Blue Light)
A shorter wavelength primarily associated with acne treatment, working through a mechanism distinct from red/NIR light — it’s been studied for its effects on the bacteria associated with acne. Devices marketed for acne specifically often include a 415nm mode in addition to red and NIR wavelengths; devices without it are typically not positioned for acne use, regardless of other wavelength capabilities. Best LED face masks for acne →
633nm / 660nm (Red Light)
The most extensively studied wavelength range for skin-level effects — collagen production, surface inflammation, and general skin health applications including rosacea and general anti-aging. 660nm specifically appears in the majority of clinical protocols for skin applications and is one half of the “660 + 850nm” pairing that shows up across most well-reviewed full-body and portable devices.
830nm / 850nm (Near-Infrared)
The deeper-penetrating counterpart to red light, associated with effects on muscle, joint, and connective tissue — this is the wavelength most relevant to applications like back pain, knee pain, and tendonitis. The 660nm vs 850nm guide explains why most well-designed protocols use both together rather than choosing one.
1072nm (Deep Near-Infrared)
A longer near-infrared wavelength used in a smaller number of devices, primarily marketed for deeper anti-aging applications in face masks. It represents one of the deepest-penetrating wavelengths commonly available in consumer devices, and is the wavelength some face masks emphasize as a differentiator for collagen-focused, anti-aging-specific use over multi-purpose masks that prioritize broader wavelength coverage instead.
What stands out: The single most useful pairing to understand is wavelength + irradiance together. I’ve seen plenty of devices with the “right” wavelength numbers on the box that don’t publish irradiance — which means there’s no way to verify the dose at the recommended distance actually matches what the research protocols used. That gap between “has the right wavelength” and “delivers a verified dose” is where a lot of the difference between devices actually lives.
The one thing I’d want to see industry-wide: Universal, third-party-verified irradiance reporting at standardized distances. Wavelength selection is usually accurate — manufacturers don’t have much reason to misstate which LEDs they’re using. Irradiance at the recommended treatment distance is the number that’s inconsistently published, and it’s the number that connects a device’s spec sheet to whether a session actually delivers a clinically meaningful dose.
Why These Terms Matter When Choosing a Device
Once you understand wavelength, irradiance, and dose as a connected system rather than three separate specs, reading any red light therapy product page gets considerably easier — and so does spotting the gaps. A listing that emphasizes wavelength count (“5 wavelengths!”) without irradiance data is telling you less than it sounds like. A listing with verified irradiance at a specific distance, paired with the 660/850nm combination that shows up across the clinical literature, is telling you more — even if the marketing copy is less exciting.
This is also the framework behind how devices are evaluated in the best red light therapy devices guide — coverage, verified wavelengths, and real total cost, rather than which spec sheet has the most numbers on it.
Frequently Asked Questions
What’s the difference between red light therapy and photobiomodulation?
They’re the same thing, described in two different contexts. “Photobiomodulation” (PBM) is the term used in peer-reviewed research and clinical literature. “Red light therapy” (RLT) is the consumer-facing term for the same mechanism — red and near-infrared light affecting cellular activity, primarily through mitochondrial pathways. If you’re reading a study, expect “PBM”; if you’re reading a product page, expect “RLT” — but they refer to the same underlying science.
What does mW/cm² actually mean for me as a buyer?
mW/cm² (milliwatts per square centimeter) measures irradiance — how intense the light is at a given distance from the device. It matters because it’s the number that, combined with session length, determines your actual dose (measured in J/cm²). A device with high irradiance at the recommended distance can deliver an adequate dose in a shorter session; a device with lower irradiance needs either a longer session or closer distance to deliver the same dose. When this number isn’t published, it’s hard to know whether the recommended protocol actually delivers a research-backed dose.
Is a higher number of wavelengths always better?
Not necessarily — it depends on what you’re treating. More wavelengths can mean more versatility (e.g., a face mask with both 415nm for acne and 633/830nm for anti-aging covers two different goals). But for a single specific goal, the relevant question is whether the right wavelength for that goal is present and delivered at sufficient irradiance — not how many total wavelengths are listed on the box. A 2-wavelength device with verified 660+850nm at adequate irradiance can outperform a 5-wavelength device where none of the wavelengths are delivered strongly enough to matter.
Does FDA clearance mean a device is clinically proven to work?
FDA Class II clearance means the device has been determined to be substantially equivalent to existing legally-marketed devices in its category — it’s primarily a safety and equivalence designation. It’s a meaningful signal (it means the device went through a real regulatory process), but it isn’t the same as the FDA independently verifying every effectiveness claim in a product’s marketing. For specific claims, checking the underlying research — which is what the main RLT guide and individual condition pages on this site link to — is the more direct way to evaluate a specific claim.
What’s the difference between a chromophore and a wavelength?
A wavelength is a property of light (measured in nanometers). A chromophore is a molecule in your body that absorbs light at specific wavelengths. The reason wavelength selection matters in device design is that different chromophores absorb different wavelengths — cytochrome c oxidase, the primary chromophore involved in photobiomodulation’s effects on mitochondria, absorbs most efficiently in specific ranges within the red and near-infrared spectrum. This is the underlying reason why 630–850nm shows up so consistently across red light therapy research, rather than the full visible light spectrum.

Cleared to use RLT? Here's where to start
